Dental
Good dental care improves your overall health. Our dental plan is designed to help you maintain a healthy smile through regular dental care and fix any problems as soon as they occur.
UnitedHealthcare (PPO 30 Network)
Lemek LLC offers you two dental plan options through UnitedHealthcare! Your dental plan provides coverage for routine exams and cleanings and pays for a portion of other services, as shown in the chart below. Go to www.myuhc.com to login for dental benefits.
Where to Find a Dentist with UnitedHealthcare
Employees and dependents have access to an extensive nationwide network of dentists through the UnitedHealthcare PPO 30 Network. The UnitedHealthcare dental plan includes both in and out-of-network coverage. You will receive the greatest cost savings by going to an in-network dentist.
In need of a dentist – visit myuhc.com. Locate an In-Network dentist by clicking on “Find a Dentist”, select Employer plans, enter your zip code, and then select “National Options PPO 30″.
Note: Employees can download a digital dental ID card via myuhc.com or through the UHC mobile app.
To request a printed copy of your card, contact UHC Member Services by calling 800-445-9090.
Dental Benefits
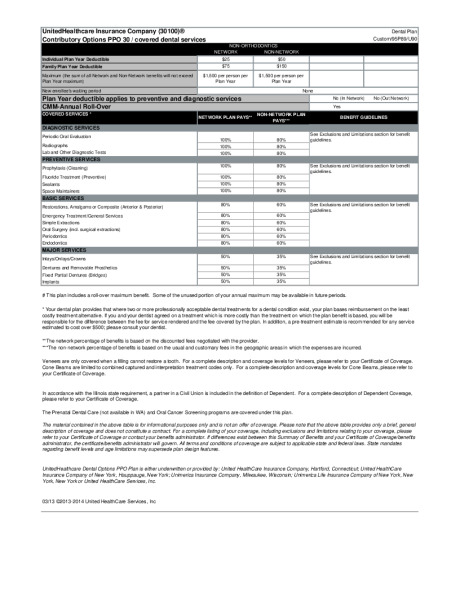
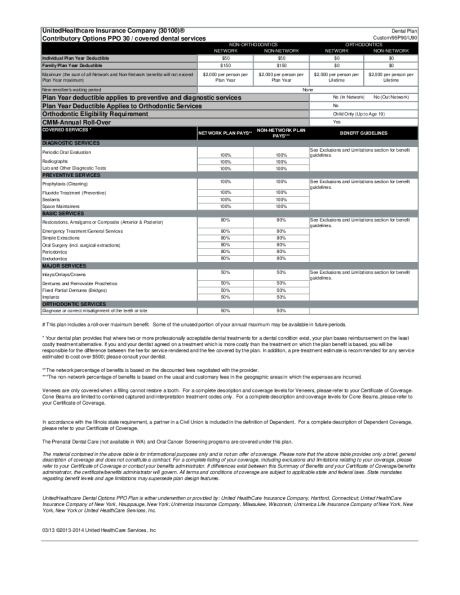
| UnitedHealthcare Dental | PPO Low | PPO High | ||||||
|---|---|---|---|---|---|---|---|---|
| In-Network (You Pay) |
Out-of-Network* (You Pay) |
In-Network (You Pay) |
Out-of-Network* (You Pay) | |||||
| Annual Deductible | ||||||||
| Individual | $25 | $50 | $50 | $50 | ||||
| Family | $75 | $150 | $150 | $150 | ||||
| Annual Maximum Benefit | ||||||||
| Per Person | $1,500 | $2,000 | ||||||
| Services | ||||||||
| Preventive and Diagnostic Care | Plan pays 100%, no deductible | Plan pays 80%, no deductible | Plan pays 100%, no deductible | Plan pays 100%, no deductible | ||||
| Basic Treatment | Plan pays 80% | Plan pays 60% | Plan pays 80% | Plan pays 80% | ||||
| Major Treatment | Plan pays 50% | Plan pays 35% | Plan pays 50% | Plan pays 50% | ||||
| Orthodontia Benefit | ||||||||
| Orthodontia Child Only | No coverage | No coverage | Plan pays 50% | Plan pays 50% | ||||
| Ortho Lifetime Maximum | No coverage | No coverage | $2,000 per person | |||||
* Balance billing may apply.
Dental Cost of Coverage
| UnitedHealthcare Dental | PPO Low | PPO High | ||
|---|---|---|---|---|
| Your Bi-monthly Deductions | ||||
| Employee Only | $5.50 | $9.00 | ||
| Employee + Spouse | $13.00 | $19.00 | ||
| Employee + Child(ren) | $15.00 | $27.00 | ||
| Employee + Family | $20.50 | $35.00 | ||
Lemek 2025 UHC PPO Low Dental Summary
Lemek 2025 UHC PPO High Dental Summary