Which Medical Plan is Right for You?
Medical insurance is essential to your well-being, and our medical coverage through UnitedHealthcare provides you and your family the protection you need for everyday health issues or when the unexpected happens.
How a Health Plan Works
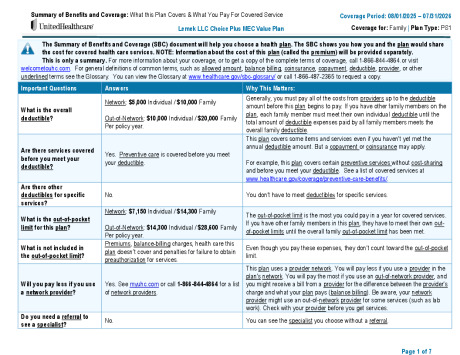
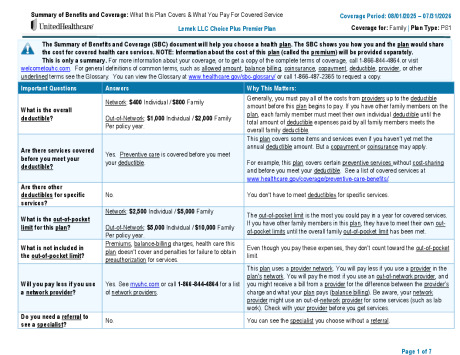
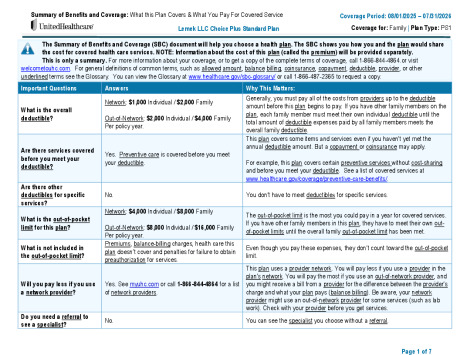
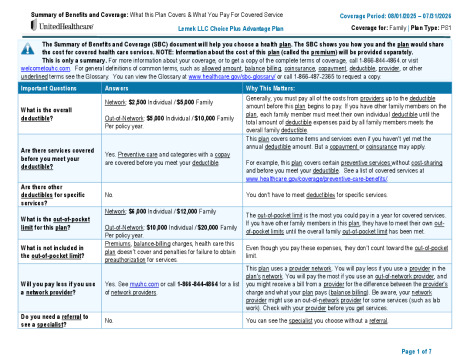
Preventive Care – like annual physical exams, vaccines and screenings – is always covered 100% when you use in-network providers. The key difference between the plans is the amount of money you’ll pay each pay period and when you need care.
The plans have different:
- Annual deductible amount – The amount you pay each year for eligible in-network and out-of-network charges before the plan begins to pay.
- Out-of-pocket maximums – The most you will pay each year for eligible network services including prescriptions. After you reach your out-of-pocket maximum, the plan picks up the full cost of covered medical care for the remainder of the plan year.
- Copays – A copay is a fixed amount you pay for a health care service. Copays do not count toward your deductible but do count toward your annual out-of-pocket maximum.
- Coinsurance – Once you’ve met your deductible, you and the plan share the cost of care, called coinsurance. For example, you may pay 20% for services and the plan will pay 80% of the cost until you have reached your out-of-pocket maximum.
Medical Plan Comparison
| UnitedHealthcare Medical | Premier Plan | Standard Plan | Advantage Plan | MEC Value Plan | ||||
|---|---|---|---|---|---|---|---|---|
| In-Network (You Pay) |
In-Network (You Pay) |
In-Network (You Pay) |
In-Network (You Pay) | |||||
| Annual Deductible | ||||||||
| Individual / Family | $400 / $800 | $1,000 / $2,000 | $2,500 / $5,000 | $5,000 / $10,000 | ||||
| Annual Out-of-Pocket Maximum | ||||||||
| Individual / Family | $2,500 / $5,000 | $4,000 / $8,000 | $6,000 / $12,000 | $7,150 / $14,300 | ||||
| Copay/Coinsurance | ||||||||
| Primary Care Physician Annual Physical | No charge | No charge | No charge | No charge | ||||
| Routine Preventive Care & Tests | No charge | No charge | No charge | No charge | ||||
| Primary Care Physician (PCP) Office Visit, Diagnostic | $20 copay | $30 copay | $40 copay | 30% | ||||
| Specialist Office Visit | $30 copay | $50 copay | $60 copay | 30% | ||||
| Diagnostic Imaging Lab Work, X-rays, MRI | 20% | 20% | 20% | 30% | ||||
|
Telemedicine Online visits through www.myuhc.com |
$10 copay | $10 copay | $10 copay | $10 copay | ||||
| Urgent Care | $30 copay | $50 copay | $60 copay | 30% | ||||
| Emergency Room Copay waived if admitted | $150 copay | $200 copay | 20% | 30% | ||||
| Inpatient Hospitalization | $250 copay then 20% | $250 copay then 20% | 20% | 30% | ||||
| Mental Health / Substance Abuse Outpatient Services | $30 copay | $50 copay | $60 copay | 30% | ||||
| Mental Health / Substance Abuse Inpatient Services | $250 copay then 20% | $250 copay then 20% | 20% | 30% | ||||
| Maternity Benefits — Includes prenatal care, delivery, postnatal care, ultrasounds, and any related complications. Refer to your plan documents for additional information. | ||||||||
| Initial Visit to Provider | $20 copay | $30 copay | $40 copay | 30% | ||||
| Childbirth/Delivery – Inpatient Hospital | $250 copay then 20% | $250 copay then 20% | 20% | 30% | ||||
Out-of-Network Benefits
| UnitedHealthcare Medical | Premier Plan | Standard Plan | Advantage Plan | MEC Value Plan | ||||
|---|---|---|---|---|---|---|---|---|
| Out-of-Network (You Pay) |
Out-of-Network (You Pay) |
Out-of-Network (You Pay) |
Out-of-Network (You Pay) | |||||
| Annual Deductible | ||||||||
| Individual / Family | $1,000 / $2,000 | $2,000 / $4,000 | $5,000 / $10,000 | $10,000 / $20,000 | ||||
| Annual Out-of-Pocket Maximum | ||||||||
| Individual / Family | $5,000 / $10,000 | $8,000 / $16,000 | $10,000 / $20,000 | $14,300 / $28,600 | ||||
Medical Bi-Monthly Contributions
| UnitedHealthcare Medical | Premier Plan | Standard Plan | Advantage Plan | MEC Value Plan | ||||
|---|---|---|---|---|---|---|---|---|
| Your Bi-monthly Deductions | ||||||||
| Employee Only | $136.00 | $87.00 | $60.00 | $35.00 | ||||
| Employee + Spouse | $306.00 | $195.00 | $166.00 | $136.00 | ||||
| Employee + Child(ren) | $278.00 | $177.00 | $150.00 | $124.00 | ||||
| Employee + Family | $435.00 | $277.00 | $235.00 | $193.00 | ||||
2025 Lemek LLC Premier Plan
2025 Lemek LLC Standard Plan
2025 Lemek LLC Advantage Plan